
In their article, “The Importance of Effective Upper Room UVGI Devices for Airborne Infection Control,” Dr. Mandar S. Sahasrabudhe, General Manager, and Dr. Avinash D Kulkarni, Chairman of Arklite Speciality Lamps (P) Ltd., emphasise the necessity of these devices in any space to ensure the safety of occupants by curbing airborne infections.
UV radiation has been known for its germicidal properties since the 19th century. Still, the recent pandemic has increased its usage in controlling microbial populations in the air to prevent airborne transmission, particularly of viruses. UV radiation is categorised into UVA, UVB, and UVC ranges, with UVC being the most effective in inactivating microbes. However, radiation from 100 to 200 nm leads to ozone formation in the air, which is toxic, so the effective range of 200 to 280 nm of UVC is used to control microbes in the air, water, and surfaces.
There are two resonance lines in its spectrum in low-pressure mercury discharge: 185 and 254 nm. Commonly used fluorescent tubes and CFLs convert these two resonance lines into visible light using a phosphor coating. However, a UV lamp is created when the phosphor is absent and the glass is transparent to UV lines. The glass used to make UV lamps block 185 nm and transmits 254 nm radiations since ozone production is not desirable in most applications. Therefore, the most commonly used UV lamps produce 254 nm UV radiation at an electrical energy to UVC radiation conversion efficiency of about 30%, much higher than a couple of percent efficiency of UVC LEDs.
The effectiveness of germicidal activity varies with wavelength, and it peaks at 265 nm, with 254 nm being very close to the peak. Therefore, its effectiveness is almost 85% of the peak value. However, a major problem with 254 nm UVC is the permissible exposure limit of 6 mJ/cm2 for eight hours per day. Far UVC sources, such as KrCl excimer lamps that produce 222 nm, are safer and have much higher exposure limits. However, these far UV sources are less efficient than mercury lamps and more expensive. Thus, the 254 nm source is a better option if a device is designed with its limitations in mind.
Precautions and recommended practice
To ensure the UV intensity of the upper room UVGI device is below 0.2 µW/ cm2 up to a height of six feet, it is necessary for a trained technician to install the device. This ensures that the total dosage over eight hours will be less than 6 mJ/cm2. Any slight misalignment during installation could result in higher UV intensity and dosage. Regular cleaning and UV intensity checks are recommended.
For the upper room UVGI device to be effective, air must be mixed between the upper and lower parts of the room. This is typically achieved automatically by convection currents in the room. Warmer air rises from the lower portion of the room and is disinfected in the upper part while the disinfected air descends. Using a ceiling fan or other types of fans can improve air movement and make the disinfection process more efficient.
Results and discussion
From a human safety perspective, designing a system that achieves a UV radiation intensity of more than 10 µW/ cm2 above six feet height and less than 0.2 µW/cm2 below six feet height is essential.
UV measurements
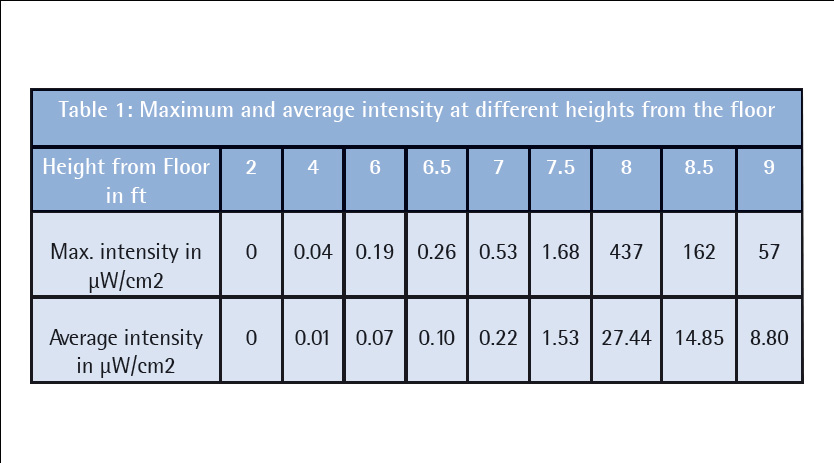
The UVGI system was installed at a height of 7.5 ft, with the system centred at 8 ft height from the floor in a room with a ceiling height of 9.5 ft, width of 12 ft, and length of 28 ft. To measure the UV intensity, 31 data points were selected at an interval of 10 cm on the left and right-hand side of the system, up to 150 cm from the centre of the system along the room’s width. These points were recorded at 1-foot intervals up to 15 feet from the system centre along the room’s length. The measurements were taken using an ILT 2400-UVGI UV meter, which has a range of 10 nW/cm2 to 500 µW/cm2 and excellent accuracy. The meter was adjusted at each point to record the maximum intensity. Table 1 shows the maximum and average intensity at each height, which were calculated from 496 different points in the plane parallel to the floor.
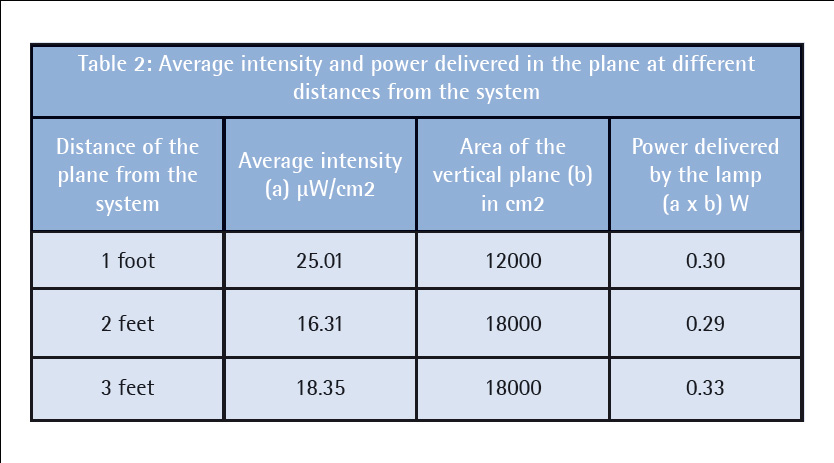
Assuming a lamp efficiency of 30 percent, meaning that only 30 percent of the electrical power input is converted into UV output, the UV power output for this lamp would be 9 W. The UV power delivered will determine the system efficiency, as shown in Table 2. If the UV power delivered by the lamp is 9 W, but the actual power delivered is only 0.31 W, then the system efficiency in UV output from the lamp is approximately 3.4 percent.
According to Table 1, the system creates an average UV intensity in the zone from 8 feet to 9 feet of 17.03µ W/cm2, which indicates that the system is well-designed according to the ASHRAE Handbook. The literature suggests that an average UV intensity of 10µ W/cm2 in the upper room can kill 63 percent of airborne tuberculosis germs that arrive within 24 seconds (equivalent to one room air change), and 99 percent within two minutes (equivalent to five room air changes).
The system can be made more effective by using a fan to circulate air in the room. The current system’s average intensity is above the ideal 10µ W/cm2, and the maximum intensities at occupant heights are within safe limits. Therefore, occupants do not need additional safety measures, such as personal protective clothing and equipment to protect their eyes and skin. However, UV measurements should be taken at heights of 6 feet and below when installing the unit at a new site to ensure occupant safety. Microbial testing was conducted to confirm the system’s effectiveness.
Microbial testing of upper room UVGI unit
To conduct microbial testing, a metal surface (SS plate) with Staphylococcus aureus bacteria was placed in the UV zone created by the upper room UVGI system. Staphylococcus aureus was selected as it requires almost double the dosage for the coronavirus, i.e., 3.9 mJ/ cm2 compared to 2 mJ/cm2 for log 1 or 90 percent reduction of the coronavirus. This dosage level has been confirmed by data reported in various papers for SARS-CoV-2 and other common respiratory viruses, as well as some modelled data based on genomic data.
The studies concluded that a dosage of 2mJ/cm2 or 2000 µJ/cm2 gives a log 1 or 90 percent reduction of aerosols in the aqueous phase. Studies done by Kowalski et al. have also shown that a dosage of 4 mJ/cm2 is useful for >log 2 reductions of influenza, smallpox, and TB bacteria.
Although the average intensities at distances higher than those measured may be higher, the actual log reduction for air disinfection will be higher than the surface disinfection data reported in Table 3, as the data was collected at specific points with lower intensities.
The >log 1 bacterial inactivation at a distance of 25 feet indicates that the system is highly efficient in an area of at least 250 sq. ft. in front of it. Although the system can be used at distances further than 25 feet, the width-wise constraint is limited to 10 feet on either side due to the design of the lamp and system.
Conclusions
UV measurements have determined that the upper room UVGI unit is well-designed to maintain high levels of UV intensity within the created UV zone, although it needs to be at the ideal level. Furthermore, from the occupants’ perspective, the unit is safe, as the UV intensity levels at 6 feet and below in the room are below the NIOSH guideline’s specified REL. Both of these design criteria are satisfactorily addressed in the current design. Microbial testing has revealed that the system is highly effective against most airborne diseases within 250 sq. ft. The study suggests that effective upper-room UVGI devices are essential in any setting to prevent airborne infections, especially in places such as doctor’s clinics and tuberculosis hospitals, where healthcare workers require protection against infections
Cookie Consent
We use cookies to personalize your experience. By continuing to visit this website you agree to our Terms & Conditions, Privacy Policy and Cookie Policy.










